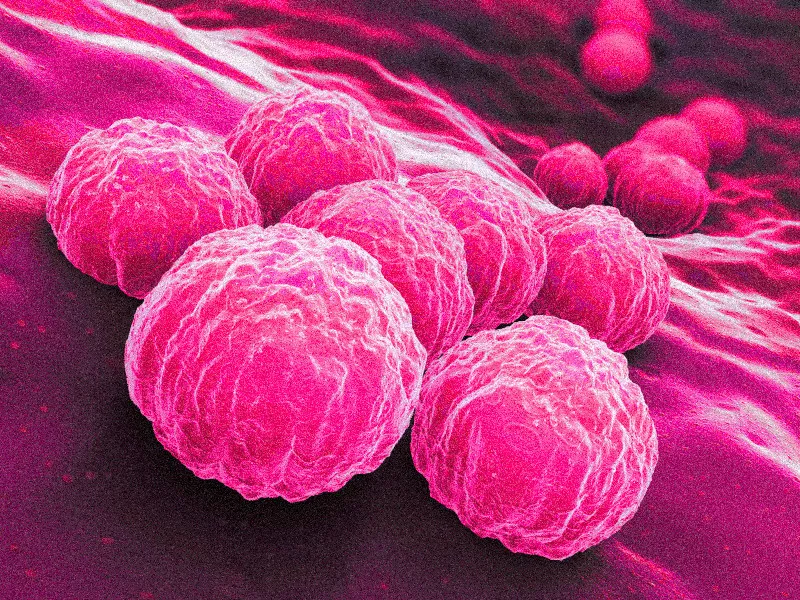
CHLAMYDIA
16173
Any sexually active person can be infected with chlamydia. It is a very common STD, especially among young people.
Chlamydia
What is chlamydia?
Chlamydia is a common sexually transmitted disease (STD) caused by infection with Chlamydia trachomatis. It can cause cervicitis in women and urethritis and proctitis in both men and women. Chlamydial infections in women can lead to serious consequences including pelvic inflammatory disease (PID), tubal factor infertility, ectopic pregnancy, and chronic pelvic pain. Lymphogranuloma venereum (LGV), another type of STD caused by different serovars of the same bacterium, occurs commonly in the developing world and has more recently emerged as a cause of outbreaks of proctitis among men who have sex with men (MSM) worldwide.
![]()
Contact us at info.bkk@pulse-clinic.com or chat on your preferred platform:
![]() +66 65 237 1936
+66 65 237 1936 ![]() @PULSEClinic
@PULSEClinic ![]() PulseClinic
PulseClinic
How common is chlamydia?
Chlamydia is the most commonly reported bacterial sexually transmitted infection (STI) in the United States. In 2014, the CDC recorded 1,441,789 cases of chlamydia from all 50 states and the District of Columbia, but it's estimated that around 2.86 million infections occur each year. A significant number of cases go unreported because many people with chlamydia do not show symptoms and do not seek testing. The infection is particularly prevalent among young individuals, with nearly two-thirds of new cases occurring in those aged 15-24. It's estimated that 1 in 20 sexually active young women aged 14-24 has chlamydia.
There are notable racial and ethnic disparities in chlamydial infection rates, with non-Hispanic blacks having a prevalence 6.7 times higher than that of non-Hispanic whites. Chlamydia is also widespread among men who have sex with men (MSM), with positivity rates for rectal chlamydial infections ranging from 3.0% to 10.5% and for pharyngeal infections ranging from 0.5% to 2.3% among those screened.
How do people get chlamydia?
Chlamydia is transmitted through sexual contact with an infected partner’s penis, vagina, mouth, or anus. It can be passed on even without ejaculation. Additionally, chlamydia can be transmitted from an untreated mother to her baby during childbirth, potentially leading to conditions like ophthalmia neonatorum (conjunctivitis) or pneumonia in some infants. Studies have shown that chlamydial conjunctivitis occurs in 18-44% and chlamydial pneumonia in 3-16% of infants born to mothers with untreated chlamydial cervical infections at the time of delivery. While rectal or genital chlamydial infections can persist for a year or more in infants infected at birth, it's important to consider the possibility of sexual abuse in prepubertal children presenting with vaginal, urethral, or rectal chlamydial infections beyond the neonatal period.
People who have been treated for chlamydia can become reinfected if they have sexual contact with someone who has the infection.
Who is at risk for chlamydia?
Any sexually active person can be infected with chlamydia. Chlamydia is a very common sexually transmitted infection (STI), particularly among young people. It is estimated that 1 in 20 sexually active young women aged 14-24 has chlamydia.
Young individuals are at a higher risk of contracting chlamydia due to a mix of behavioral, biological, and cultural factors. Many do not use condoms consistently, and some adolescents may transition quickly between monogamous relationships, increasing the likelihood of transmission during the infection's window. Additionally, teenage girls and young women may experience cervical ectopy, where cells from the endocervix are found on the ectocervix, which can make them more susceptible to chlamydia. The higher prevalence among young people may also be attributed to various barriers to accessing STI prevention services, such as transportation issues, cost, and stigma.
Men who have sex with men (MSM) are also at risk for chlamydial infection since it can be transmitted through oral or anal sex. Among MSM screened for rectal chlamydial infections, positivity rates range from 3.0% to 10.5%, while rates for pharyngeal infections range from 0.5% to 2.3%.
What are the symptoms of chlamydia?
Chlamydia is known as a ‘silent’ infection because most infected people are asymptomatic and lack abnormal physical examination findings. Estimates of the percentage of chlamydia-infected individuals who show symptoms vary based on the setting and study methods used. Two published studies that employed modeling techniques to address the limitations of point prevalence surveys suggested that only about 10% of men and 5-30% of women with laboratory-confirmed chlamydial infections develop symptoms. The incubation period for chlamydia is not well defined, but due to the organism's relatively slow replication cycle, symptoms may not appear until several weeks after exposure for those who do become symptomatic.
In women, the bacteria initially infect the cervix, potentially leading to signs of cervicitis, such as mucopurulent endocervical discharge and easily induced bleeding. The infection can also affect the urethra, causing symptoms of urethritis, including pyuria, dysuria, and increased urinary frequency. If the infection spreads from the cervix to the upper reproductive tract (the uterus and fallopian tubes), it can result in pelvic inflammatory disease (PID), which may be asymptomatic (referred to as “subclinical PID”) or acute, presenting with abdominal or pelvic pain, along with tenderness on examination.
Men with symptoms typically experience urethritis, characterized by a mucoid or watery discharge and dysuria. A smaller percentage of infected men may develop epididymitis, which can occur with or without symptomatic urethritis and is marked by unilateral testicular pain, tenderness, and swelling.
Chlamydia can also infect the rectum in both men and women, either directly through receptive anal sex or potentially through spread from the cervix and vagina in women with cervical infections. Although these rectal infections are often asymptomatic, they can lead to symptoms of proctitis, such as rectal pain, discharge, and bleeding.
Sexually transmitted chlamydial conjunctivitis can occur in both men and women through contact with infected genital secretions.
While chlamydia may also be present in the throats of men and women who engage in oral sex with an infected partner, it is usually asymptomatic and is not considered a significant cause of pharyngitis.
What complications can result from chlamydial infection?
The initial damage that chlamydia causes often goes unnoticed. However, chlamydial infections can lead to serious health problems with both short- and long-term consequences.
In women, untreated chlamydia can spread into the uterus or fallopian tubes and cause pelvic inflammatory disease (PID). Symptomatic PID occurs in about 10 to 15 percent of women with untreated chlamydia. However, chlamydia can also cause subclinical inflammation of the upper genital tract (“subclinical PID”). Both acute and subclinical PID can cause permanent damage to the fallopian tubes, uterus, and surrounding tissues. The damage can lead to chronic pelvic pain, tubal factor infertility, and potentially fatal ectopic pregnancy.
Some patients with chlamydial PID develop perihepatitis, or “Fitz-Hugh-Curtis Syndrome”, an inflammation of the liver capsule and surrounding peritoneum, which is associated with right upper quadrant pain.
In pregnant women, untreated chlamydia has been associated with pre-term delivery, as well as ophthalmia neonatorum (conjunctivitis) and pneumonia in the newborn.
Reactive arthritis can occur in men and women following symptomatic or asymptomatic chlamydial infection, sometimes as part of a triad of symptoms (with urethritis and conjunctivitis) formerly referred to as Reiter’s Syndrome.
What about chlamydia and HIV?
Untreated chlamydia may increase a person’s chances of acquiring or transmitting HIV – the virus that causes AIDS.
How does chlamydia affect a pregnant woman and her baby?
In pregnant women, untreated chlamydia has been linked to preterm delivery and can lead to ophthalmia neonatorum (conjunctivitis) and pneumonia in newborns. Studies have shown that chlamydial conjunctivitis occurs in 18-44% and chlamydial pneumonia in 3-16% of infants born to mothers with untreated chlamydial cervical infections during delivery. Routine neonatal prophylaxis against gonococcal conjunctivitis does not effectively prevent chlamydial conjunctivitis.
The best way to prevent neonatal chlamydial disease is through the screening and treatment of chlamydia in pregnant women. All pregnant women should be screened for chlamydia during their first prenatal visit. Those under 25 and those at higher risk for chlamydia (such as women with new or multiple sexual partners) should be screened again in their third trimester. Pregnant women with chlamydial infection should be retested three weeks and three months after completing the recommended treatment.
Who should be tested for chlamydia?
Any sexually active person can contract chlamydia. People experiencing genital symptoms such as discharge, burning during urination, unusual sores, or rashes should avoid sexual activity until they can consult a healthcare provider.
Additionally, anyone who has had oral, anal, or vaginal sex with a partner recently diagnosed with an STD should seek evaluation from a healthcare provider.
Since chlamydia is often asymptomatic, regular screening is essential for identifying most infections. Screening programs have been shown to decrease the incidence of adverse outcomes in women. The CDC recommends annual chlamydia screening for all sexually active women under 25, as well as for older women with risk factors like new or multiple partners or a partner with a sexually transmitted infection. Pregnant women should be screened at their first prenatal visit, and those under 25 or at increased risk (such as those with new or multiple partners) should be screened again during their third trimester. Women diagnosed with chlamydia should be retested approximately three months after treatment. All sexually active women should discuss their risk factors with a healthcare provider to determine if more frequent screening is needed.
Routine screening is not recommended for men, but sexually active young men in clinical settings with a high prevalence of chlamydia (such as adolescent clinics, correctional facilities, and STD clinics) should be considered for screening, provided it does not interfere with screening efforts for women.

Sexually active men who have sex with men (MSM) who had insertive intercourse should be screened for urethral chlamydial infection and MSM who had receptive anal intercourse should be screened for rectal infection at least annually; Screening for pharyngeal chlamydial infection is not recommended. However, more frequent chlamydia screening every three months is advised for men who have sex with men (MSM), including those with HIV, if they continue engaging in risky behaviors or if they or their sexual partners have multiple partners.
During the initial HIV care visit, healthcare providers should test all sexually active individuals with HIV for chlamydia and continue testing at least annually while they are in HIV care. The healthcare provider may recommend more frequent screenings based on the patient’s specific risk factors.
How is chlamydia diagnosed?
There are various diagnostic tests for chlamydia, including nucleic acid amplification tests (NAATs), cell cultures, and others. NAATs are the most sensitive tests and can be performed on easily collected specimens, such as vaginal swabs (either clinician- or patient-collected) or urine.
For women, vaginal swabs—whether collected by the patient or clinician—are the preferred specimen for screening genital chlamydia using NAATs. For men, urine is the specimen of choice and also serves as an effective alternative for women. Self-collected vaginal swab specimens are at least as reliable as other approved specimens when using NAATs. Additionally, patients may prefer self-collected vaginal swabs or urine-based screening over more invasive endocervical or urethral swabs. Adolescent girls, in particular, may benefit from self-collected vaginal swabs or urine-based screening, as pelvic exams are unnecessary if they are asymptomatic.
Chlamydial cultures can be used for rectal or pharyngeal specimens but are not widely available. NAATs have shown improved sensitivity and specificity compared to cultures for detecting C. trachomatis at non-genital sites. While most tests, including NAATs, are not FDA-cleared for use with rectal or pharyngeal swabs, some laboratories have met regulatory requirements and validated NAAT testing for these sites.
Chlamydial DNA can be detected on urine samples, painless throat/anal/vaginal swab with PCR DNA Test Multiplex. The correct type of antibiotics can treat chlamydia (which you can get at PULSE clinics). If you do require treatment for chlamydia your partner will too. Otherwise, you may contract it again.
PCR Multiplex DNA Test for 28 Infections 
Our STD PCR Multiplex test offers advanced technology to detect up to 28 infections, including Gonorrhea, Chlamydia, Syphilis, Herpes Simplex, Trichomonas, and Candida strains, all in one test. It can identify infections in various anatomical areas, such as the throat, urethra, anorectal region, vagina, cervix, sperm, and skin lesions. For urethral infections, the Urine PCR is recommended, while the Throat Swab PCR is ideal after oral sex. Anal Swab PCR is advised for unprotected anal sex, and the Vaginal Swab PCR is recommended for vaginal sex, with staff guidance available for all tests.
| PCR for 28 Infections (STD Multiplex) | Online results | |||
| Same day** | Next day | 3 days | 7 days | |
| Throat | 14,000 THB | 11,600 THB | 10,480 THB | 9,200 THB |
| Urine | 14,000 THB | 11,600 THB | 10,480 THB | 9,200 THB |
| Anal Swab | 14,000 THB | 11,600 THB | 10,480 THB | 9,200 THB |
| Vaginal Swab | 14,000 THB | 11,600 THB | 10,480 THB | 9,200 THB |
| Cervical Swab | 14,000 THB | 11,600 THB | 10,480 THB | 9,200 THB |
| Sperm | 14,800 THB | 12,640 THB | 11,600 THB | 10,080 THB |
| Skin Lesion Swab | 14,000 THB | 11,600 THB | 10,480 THB | 9,200 THB |
| Pooling | 15,600 THB | 13,280 THB | 12,400 THB | 10,800 THB |
| PCR for 2 Infections (Gonorrhea/Chlamydia) | Same day | Next day | 3 days | 7 days |
| Throat | 5,690 THB | 4,990 THB | 3,990 THB | 3,300 THB |
| Urine | 5,690 THB | 4,990 THB | 3,990 THB | 3,300 THB |
| Vaginal and Cervical Swab | 5,690 THB | 4,990 THB | 3,990 THB | 3,300 THB |
| Rectal Swab | 5,690 THB | 4,990 THB | 3,990 THB | 3,300 THB |
| Sperm* | 6,200 THB | 5,150 THB | 4,100 THB | 3,690 THB |
| Skin lesion Swab | 5,690 THB | 4,990 THB | 3,990 THB | 3,300 THB |
![]()
Contact us at info.bkk@pulse-clinic.com or chat on your preferred platform:
![]() +66 65 237 1936
+66 65 237 1936 ![]() @PULSEClinic
@PULSEClinic ![]() PulseClinic
PulseClinic
How long does it take for Chlamydia to go away? What is the treatment for chlamydia?
Chlamydia can be easily cured with antibiotics. HIV-positive persons with chlamydia should receive the same treatment as those who are HIV-negative.
Persons with chlamydia should abstain from sexual activity for 7 days after single dose antibiotics or until completion of a 7-day course of antibiotics, to prevent spreading the infection to partners. It is important to take all of the medication prescribed to cure chlamydia. Medication for chlamydia should not be shared with anyone. Although medication will cure the infection, it will not repair any permanent damage done by the disease. If a person’s symptoms continue for more than a few days after receiving treatment, he or she should return to a healthcare provider to be reevaluated.
Repeat infection with chlamydia is common. Women whose sex partners have not been appropriately treated are at high risk for re-infection. Having multiple chlamydial infections increases a woman's risk of serious reproductive health complications, including pelvic inflammatory disease and ectopic pregnancy. Women and men with chlamydia should be retested about three months after treatment of an initial infection, regardless of whether they believe that their sex partners were successfully treated.
Infants infected with chlamydia may develop ophthalmia neonatorum (conjunctivitis) and/or pneumonia. Chlamydial infection in infants can be treated with antibiotics.
What about partners?
If someone has been diagnosed and treated for chlamydia, they should inform all recent anal, vaginal, or oral sex partners (specifically, partners within the 60 days before the onset of symptoms or diagnosis) so that those partners can see a healthcare provider and receive treatment. This helps reduce the risk of serious complications for the partners and lowers the likelihood of the original person becoming re-infected. Both the person with chlamydia and their partners should avoid sexual activity until they have completed their treatment (i.e., seven days after a single dose of antibiotics or until finishing a seven-day course) and until they no longer have symptoms.
To help get partners treated quickly, healthcare providers in some states may give infected individuals extra medicine or prescriptions to give to their sex partners. This is called expedited partner therapy or EPT. In published clinical trials comparing EPT to traditional patient referral (i.e., asking the patient to refer their partners for treatment), EPT was associated with fewer persistent or recurrent chlamydial infections in the index patient, and a larger reported number of partners treated. For providers, EPT represents an additional strategy for partner management of persons with chlamydial infection; partners should still be encouraged to seek medical evaluation, regardless of whether they receive EPT. To obtain further information regarding EPT, including the legal status of EPT in a specific area, see the Legal Status of Expedited Partner Therapy.
Window period of CHLAMYDIA
The window period for chlamydia refers to the time between initial exposure to the bacteria Chlamydia trachomatis and when it can be detected through testing. Typically, this window period ranges from 1 to 3 weeks.
During this time, a person may not show symptoms, but the infection could still be present and transmissible to others. Testing is most reliable about 2 weeks after possible exposure, as it allows enough time for the bacteria to reach detectable levels. However, if symptoms like unusual discharge, pain during urination, or pelvic pain develop earlier, testing should be done immediately.
How can chlamydia be prevented?
Latex male condoms, when used consistently and correctly, can significantly lower the risk of contracting or transmitting chlamydia. The most effective way to prevent chlamydia is to abstain from vaginal, anal, and oral sex or to maintain a long-term, mutually monogamous relationship with a partner who has been tested and is confirmed to be uninfected.
PULSE Teleconsult: Connect with Doctors Anytime, Anywhere!
PULSE now offers PULSE Telemedicine & Teleconsult, enabling both new and existing patients to connect with doctors over 20 branches across 6 countries during clinic hours for non-emergency consultations. After the consultation, medications are delivered directly to the patient's doorstep.
3 Easy Steps to Get a Teleconsult with PULSE!
- Connect with us Either on WhatsApp, or Line App to Chat with us or call us to talk with our staff to request teleconsult.
- Verification & Consultation Our team will guide you through the verification process before your online consultation. Our doctors provide virtual consultations via available platforms, just like a traditional visit—only from the comfort of your home! Access care anywhere, anytime.
- Get Your Treatment From Home! If your doctor determines that medication is necessary, they will provide you with a medical certificate and prescription. Your medication can be delivered to your address through our online delivery service, or in some cases, you may choose to use the prescription at a local pharmacy. For certain conditions, further lab tests may be required, and the doctor may recommend scheduling an appointment at one of our clinics near you!
Test of Cure After Treatment with Our Teleconsult Services: Ensuring Complete Recovery
After completing treatment through our teleconsult services, your doctor may recommend a PCR test as a follow-up test of cure. This is to ensure the effectiveness of the treatment and that the prescribed medication has successfully eliminated the infection. We prioritize your health by confirming that no infection remains in your system, helping to prevent persistent or recurrent infections, complications, or the development of drug resistance. Typically, this test is performed around three weeks after your final day of treatment to ensure optimal results.
Teleconsult is now available for booking through our staff at PULSE Clinic. Our team will help guide you through the process to ensure your session with one of our doctors goes as smoothly as possible for you. Contact us at info.bkk@pulse-clinic.com or chat on your preferred platform:
Trusted by over 100,000 patients from more than 196 countries and regions, PULSE CLINIC provides discreet, professional healthcare with privacy and respect at every step. Here to Help. Not to Judge!
Add us on Line and stay in touch.
Loading...
Clinic Locations
Loading...